Management
Post-coital bleeding (1)
History:
- Frequency, severity and duration of symptoms
- Current contraception
- Smear History: regular, irregular, including date and result of last smear
- Details of previous colposcopy, any treatments such as LLETZ/cold coagulation/laser
- Relevant past medical/surgical history (including haematological/ coagulation disorders)
- Current regular medication
- It is imperative to also screen patients for domestic abuse and/or sexual abuse as genital tract trauma can lead to postcoital bleeding
Examination:
- Examination of vulva, vagina and cervix with a speculum for abnormal findings (e.g. normal, ectropion, cervicitis, cervical polyp, trauma, ulceration)
Investigations prior to referral:
- Investigation results: Chlamydia and full STI screening, pregnancy test
Treatment of Ectopy
- cervical ectropion can be caused by hormone imbalance, pregnancy or the pill. It does not require treatment unless bleeding is persistent and bothersome to the patient. Prior to proceeding with treatment, one should ensure that they have ruled out underlying malignancy as certain treatments for cervical ectropion may mask or exacerbate malignant lesions
- consider changing the type of contraceptive used
- an alternative therapy may be to use acidifying agents such as boric acid suppositories 600 mg vaginally at bedtime, Relactagel or Balance Active vaginally. Cervical ablation with either cryotherapy or electrocautery is effective in mitigating further postcoital bleeding and a routine referral can be made for this to secondary care. However, there are significant side effects to include copious vaginal discharge until healing is complete and cervical stenosis which can affect subsequent pregnancies
2WW Cancer Referral (2)
If cervix appears suspicious of malignancy on examination or if the pattern of bleeding is suspicious – refer under 2WW suspected cancer referral system.
Red flags:
• Suspicious looking cervix
• Suspicious vulval lesion
• Suspicious vaginal mass
- Take a cervical smear only if a woman is due or overdue for her regular screening.
- No additional smear tests should be performed where the patient is not due a repeat.
- Negative smear test should not stop referral.
- Referral should not be delayed for results of smear when cancer is suspected
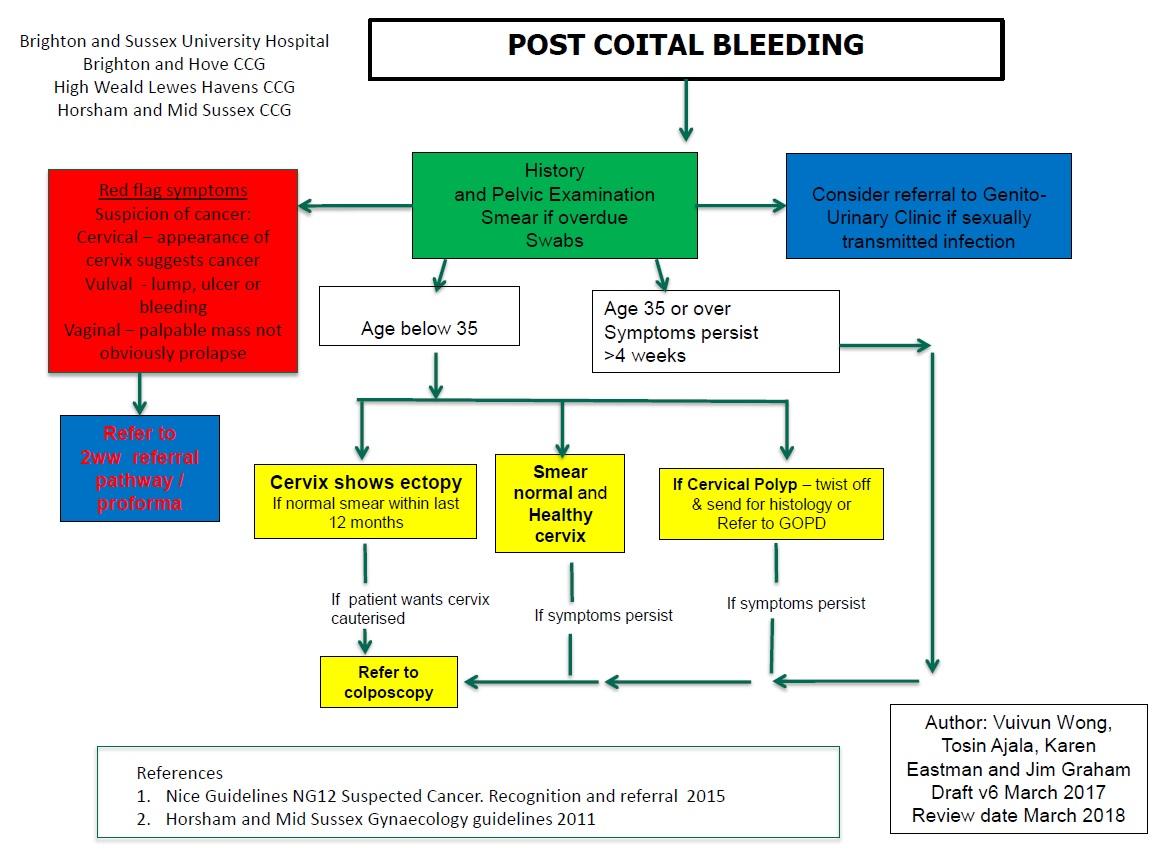
A useful algorithm regarding general principles of management in this condition is presented below:
Reference:
- Owens G et al. Investigation and management of postcoital bleeding. The Obstetrician & Gynaecologist. 2022;24:24–30
- Suspected cancer: recognition and referral. NICE guideline [NG12] Published: 23 June 2015 Last updated: 02 October 2023
Create an account to add page annotations
Add information to this page that would be handy to have on hand during a consultation, such as a web address or phone number. This information will always be displayed when you visit this page