Management of cow's milk protein allergy
Dietary advice:
IgE mediated cow's milk protein allergy
- managed via secondary care - a diet free from cow’s milk protein. Exclude all cow’s milk and products
non-IgE mediated cow's milk protein allergy
- Dietary management involves removing the allergenic protein from the diet
- all dairy products must be removed from the diet of a breastfeeding mother if milk allergy is suspected in the infant and calcium supplements given
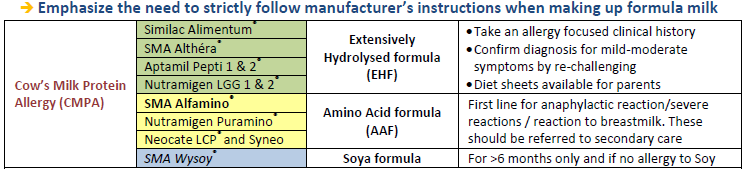
- in a formula-fed infant, choice of formula is determined by the severity of the symptoms
- most infants respond to extensively hydrolysed formulas, where the milk protein is broken down
- amino acid formulas should be reserved for severe symptoms and those not responding to an extensively hydrolysed formula
- should also be used first line if top-up feeds are required in an infant who is exclusively breast fed and shows symptoms suggestive of cow’s milk allergy
- acquisition of tolerance in cow’s milk allergy should be considered after at least 6 months on a diet free from milk protein
- likely that tolerance to extensively baked milk products will occur before that to less well cooked milk
- refer to secondary care only if symptoms severe (4)
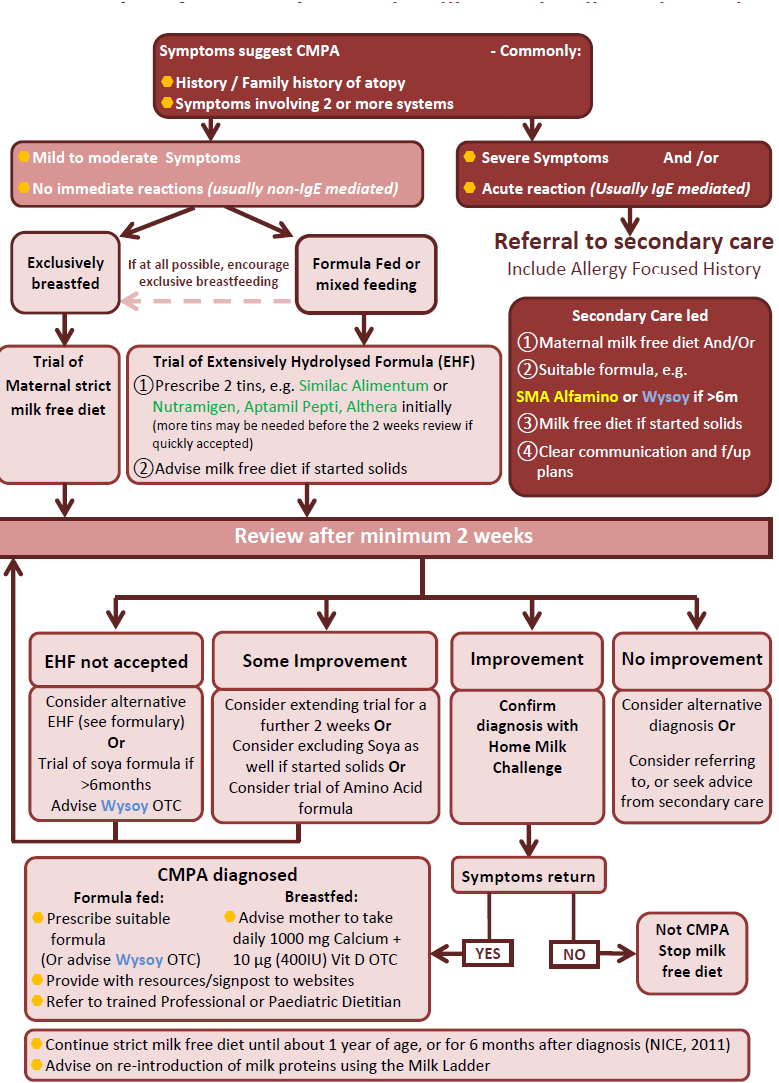
Flow chart for managing cow's milk protein allergy:
Prescribing information:
Cow’s Milk Protein Allergy additional notes (1,2,3)
- soya is not recommended before 6 months of age due to it containing isoflavones, which may exert a weak oestrogenic effect. There is also a risk of cross-reactivity: up to 14% of those with IgE-mediated cow’s milk allergy also react to soya and up to 60% of those with non-IgE-mediated cow’s milk allergy
- rice milk is not recommended in those aged <4.5 years due to the arsenic content; and there is cross-reaction between mammalian milks
- goat’s milk and products are not suitable for infants with cow’s milk allergy
- breastfeeding is the optimal way to feed a baby with CMPA, with, if required, individualised maternal elimination of all cow’s milk protein foods (+ Calcium and vitamin D supplementation).
- CMPA commonly appear when a formula is introduced in a usually breastfed baby. Therefore returning to exclusive breastfeeding should be discussed and encouraged at the earliest opportunity
- in the UK, 2-3% of 1-3year olds have confirmed CMPA (the highest prevalence in Europe)
- only about 10% of babies with CMPA will require an AAF (amino-acid free). The remainder should tolerate an EHF
- 10-14% of infant with CMPA will also react to soya proteins (and up to 50% of those with non-IgE mediated CMPA). But because of better palatability soya formula is worth considering in babies>6months
Reference:
- Walsh J et al. Differentiating milk allergy (IgE and non-IgE mediated) from lactose intolerance: understanding the underlying mechanisms and presentations. Br J Gen Pract 2016; DOI: 10.3399/bjgp16X686521
- Ludman S, Shah N, Fox AT. Managing cow’s milk allergy in children. BMJ 2013; 347: f5424.
- Wessex Infant Feeding Guidelines and Appropriate Prescribing of Specialist Infant Formulae (Accessed 8/3/2020)
- NHS Fife. Diagnosis and Management of Infants with Suspected Cow’s Milk Protein Allergy. A guide for healthcare professionals working in primary care (Accessed 8/3/2020)
Create an account to add page annotations
Annotations allow you to add information to this page that would be handy to have on hand during a consultation. E.g. a website or number. This information will always show when you visit this page.