Follow up after curative resection for colorectal cancer
Follow-up after apparently curative resection
- start follow-up at a clinic visit 4-6 weeks after potentially curative treatment
- offer patients regular surveillance with:
- a minimum of two CTs of the chest, abdomen, and pelvis in the first 3 years and
- regular serum carcinoembryonic antigen tests (at least every 6 months in the first 3 years) (1)
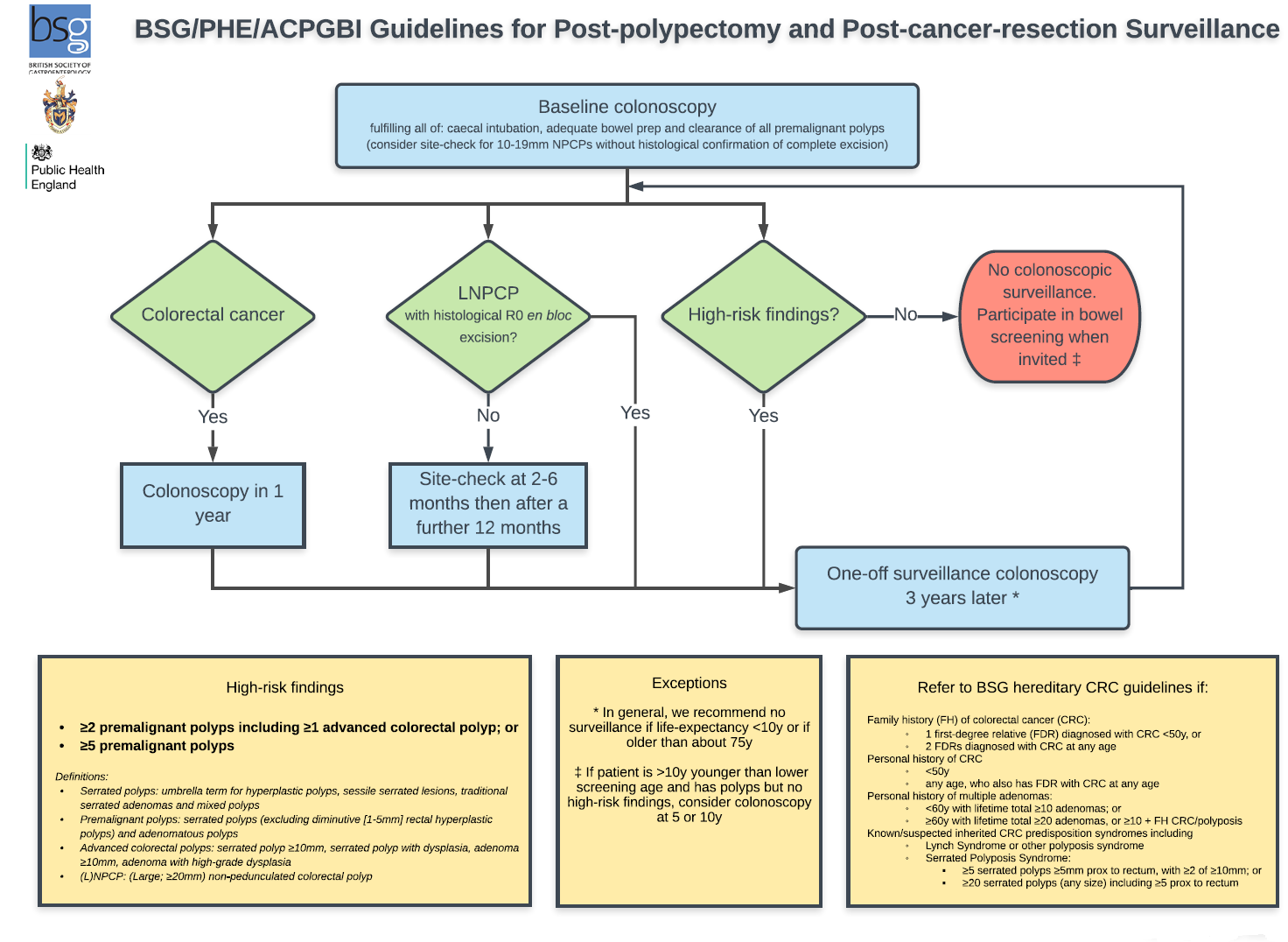
Consensus guidelines have been developed by the British Society of Gastroenterology, the Association of Coloproctology of Great Britain and Ireland and Public Health England (2)
Key recommendations are that the high-risk criteria for future colorectal cancer (CRC) following polypectomy comprise EITHER:
- 2 or more premalignant polyps including at least one advanced colorectal polyp (defined as a serrated polyp of at least 10mm in size or containing any grade of dysplasia, or an adenoma of at least 10mm in size or containing high-grade dysplasia);
- OR
- 5 or more premalignant polyps
- start reinvestigation if there is any clinical, radiological or biochemical suspicion of recurrent disease
Reference:
- NICE. Colorectal cancer (management in people aged 18 and over). NG151. 2020, updated December 2021
- BSG/ACPGBI/PHE (September 2019).Post-polypectomy and post-colorectal cancer resection surveillance guidelines.
Related pages
Create an account to add page annotations
Annotations allow you to add information to this page that would be handy to have on hand during a consultation. E.g. a website or number. This information will always show when you visit this page.