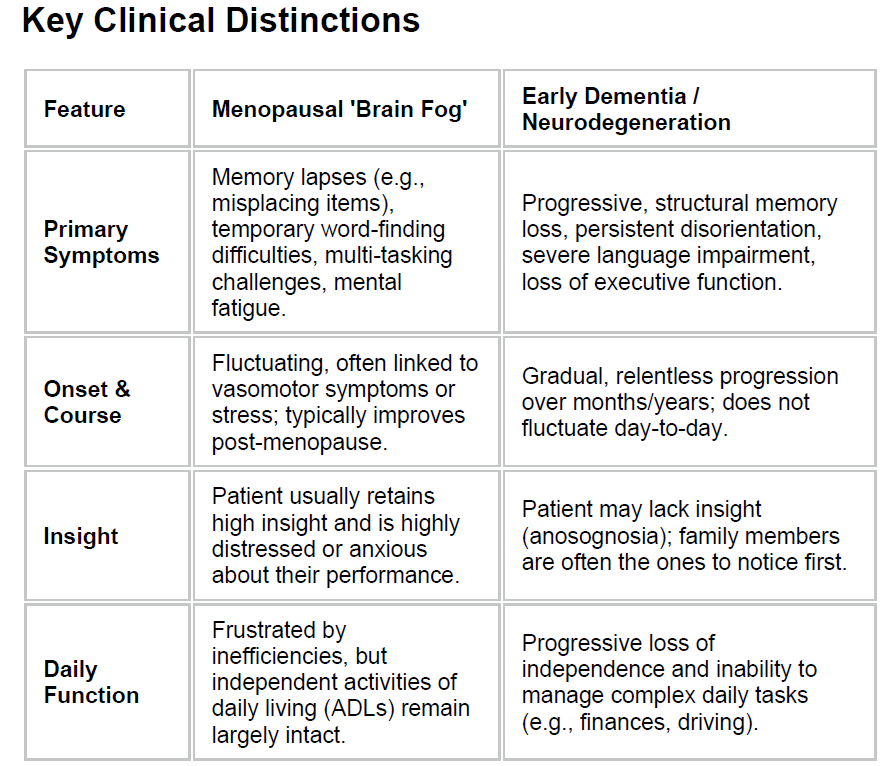
discriminating menopausal 'brain fog' from dementia
The menopause transition interacts with sleep disruption, vasomotor symptoms, stress physiology, mood changes, and competing life demands characteristic of midlife, potentially amplifying day-to-day variability in attention and memory processes (1).
Cognitive symptoms - collectively termed ‘brain fog’ are highly prevalent during the perimenopause and menopause transition (2).
‘Brain fog’ has been defined as (2):
- self-reported impairment in one or more cognitive areas (such as memory, attention, organisation, problem solving, word retrieval) in the absence of a significant, objective cognitive decline
- can fluctuate (for example daily or across a menstrual cycle) and cause mild to significant distress and impact on quality of life
- does not result in sustained changes in capacity to perform activities of daily living
- the most common cognitive symptoms are subjective (or self-reported) symptoms such as:
- losing a train of thought
- word finding difficulties
- loss of immediate focus (what was meant to be done)
- forgetting information
- distraction
- misplacement of items
- difficulties on multitasking
- these symptoms often cause severe patient distress and can be mistaken by patients (and clinicians) for early-onset dementia
- differentiating benign, transition-related cognitive fluctuation from neurodegenerative disease is crucial for appropriate reassurance, investigation, and management
Practical approach
History and assessment of cognitive assessments (2)
- discuss age of onset, duration and nature of the problem (sudden vs insidious; fluctuating vs progressive)
- consider the context (any menstrual changes, HRT use, associated with other menopause symptoms)
- ask about impact: work/functional impact
- check family history of neurodegenerative disease
- ask about alcohol consumption, smoking and any other substance use
- assess and address vascular risk factors
- rule out other medical conditions, nutritional deficiencies, psychiatric conditions and psychosocial factors that could contribute to or exacerbate cognitive symptoms during midlife.
- consider sleep quality
- assess sleep (sleep apnoea, disrupted sleep and insomnia) as well as vasomotor symptoms – which can all exacerbate cognitive symptoms directly or indirectly
- chronic sleep disruption (often driven by nocturnal vasomotor symptoms/night sweats) directly compromises daytime executive function and memory consolidation
- assess sleep (sleep apnoea, disrupted sleep and insomnia) as well as vasomotor symptoms – which can all exacerbate cognitive symptoms directly or indirectly
- review medication - concomitant use of sedative-hypnotics, anticholinergics, or polypharmacy affecting central nervous system function
- suggested blood tests include full blood count, thyroid function, vitamin deficiencies such as B12, folate, vitamin D, HBA1C, liver and kidney function and inflammatory markers
- consider sleep quality
Management overview:
Treat contributing modifiable risk factors
- manage mood, sleep and vasomotor symptoms – consider HRT, psychological therapies (CBT or other talking therapies)
- review medications and consider a test for thyroid disease, B12 deficiency
- diabetes management
- monitor vascular risk factors and treat accordingly
- encourage physical activity, good hydration and stress reduction strategies
- promote regular aerobic exercise, stress-reduction techniques (mindfulness, yoga), a balanced diet, and cognitive engagement
When to refer
- atypical features such as neurological signs, seizures, rapid progression
- significant and sudden decline, risk to safety
- family history of early onset (under 65) cognitive impairment/dementia
- objective cognitive deficits confirmed on validated screening tools (e.g., GPCOG)
- cognitive symptoms are progressive and/or interfere substantially with work performance, relationships or quality of life
Reference:
- Gazerani P. Menopause-related brain fog as a midlife window in women's brain aging: toward ecologically valid measurement and digital phenotyping. Front Hum Neurosci. 2026 Apr 21;20:1814092.
- British Menopause Society (June 2026). Menopausal ‘brain fog’ or dementia? – a practical guide for clinicians.
Related pages
Create an account to add page annotations
Annotations allow you to add information to this page that would be handy to have on hand during a consultation. E.g. a website or number. This information will always show when you visit this page.