Management of chronic asthma in individuals aged 12 years and over
The aim of asthma management is control of the disease. Complete control is defined as
- no daytime symptoms
- no night-time awakening due to asthma
- no need for rescue medication
- no asthma attacks
- no limitations on activity including exercise
- normal lung function (in practical terms FEV1 and/or PEF >80% predicted or best)
- minimal side effects from medication
NICE guidance states (1):
Initial management of newly diagnosed asthma in people aged 12 and over
- a low-dose inhaled corticosteroid (ICS)/formoterol combination inhaler should be offered to be taken as needed for symptom relief (as-needed AIR therapy) to people aged 12 and over with newly diagnosed asthma
- Anti-inflammatory reliever (AIR) therapy
- is treatment with a reliever inhaler that contains a combination of an inhaled corticosteroid and formoterol
- when this is used in response to symptoms without regular maintenance therapy it is called as-needed AIR therapy
- Anti-inflammatory reliever (AIR) therapy
- if the person needing asthma treatment presents highly symptomatic (for example, regular nocturnal waking) or with a severe exacerbation, start treatment with low-dose MART (maintenance and reliever therapy) in addition to treating the acute symptoms as indicated (that is, a course of oral corticosteroids may be needed)
- consider stepping down to as-needed AIR therapy using a low-dose ICS/formoterol inhaler at a later date if their asthma is controlled
- Maintenance and reliever therapy (MART)
- a form of combined ICS plus formoterol treatment in which a single inhaler containing ICS and formoterol is used for daily maintenance therapy and the relief of symptoms as needed
- the terms low-dose MART and moderate-dose MART refer to the dosage of the maintenance component of MART
- people using MART do not normally need a SABA
Medicine combination and sequencing in people aged 12 and over
- low-dose MART should be offered to people aged 12 and over with asthma that is not controlled on a low-dose ICS/formoterol combination inhaler used only as needed
- moderate-dose MART should be offered to people aged 12 and over with asthma that is not controlled on low-dose MART
If aged 12 and over with asthma that is not controlled on moderate-dose MART despite good adherence then:
- check the fractional exhaled nitric oxide (FeNO) level if available, and the blood and if either is raised then refer to a specialist in asthma care
- if neither FeNO or eosinophil count is raised, consider a trial of either a leukotriene receptor antagonist (LTRA) or a long-acting muscarinic receptor antagonist (LAMA) used in addition to moderate-dose MART
- the medicine should be given for a trial period of 8 to 12 weeks unless there are side effects. At the end of the trial:
- if asthma is controlled, continue the treatment
- if control has improved but is still inadequate, continue the treatment and start a trial of the other medicine (LTRA or LAMA)
- if control has not improved, stop the LTRA or LAMA and start a trial of the alternative medicine (LTRA or LAMA)
- the medicine should be given for a trial period of 8 to 12 weeks unless there are side effects. At the end of the trial:
Refer people to a specialist in asthma care when asthma is not controlled despite treatment with moderate-dose MART, and trials of an LTRA and a LAMA.
Transferring people aged 12 and over from other treatment pathways:
Recommendations are for people with uncontrolled asthma who are on the treatment pathway recommended by previous NICE and BTS/SIGN guidelines.
- change treatment for people with confirmed asthma who are currently using a short-acting beta2 agonist (SABA) only to a low-dose ICS/formoterol combination inhaler used as needed (as-needed AIR therapy)
- changing treatment to low-dose MART should be considered for people with asthma that is not controlled on:
- regular low-dose ICS plus SABA as needed
- regular low-dose ICS/LABA combination inhaler plus SABA as needed
- regular low-dose ICS and supplementary therapy (LTRA) plus SABA as needed.
- regular low-dose ICS/LABA combination inhaler and supplementary therapy (LTRA) plus SABA as needed
- changing treatment to moderate-dose MART should be considered for people with asthma that is not controlled on:
- regular moderate-dose ICS plus SABA as needed
- regular moderate-dose ICS/LABA combination inhaler plus SABA as needed
- regular moderate-dose ICS and supplementary therapy (LTRA or LAMA, or both) plus SABA as needed
- regular moderate-dose ICS/LABA combination inhaler and supplementary therapy (LTRA or LAMA, or both) plus SABA as needed.
When changing from low- or moderate-dose ICS (or ICS/LABA combination inhaler) plus supplementary therapy to MART, consider whether to stop or continue the supplementary therapy based on the degree of benefit achieved when first introduced
Refer people with asthma that is not controlled on treatment containing a high dose of ICS to a specialist in asthma care.
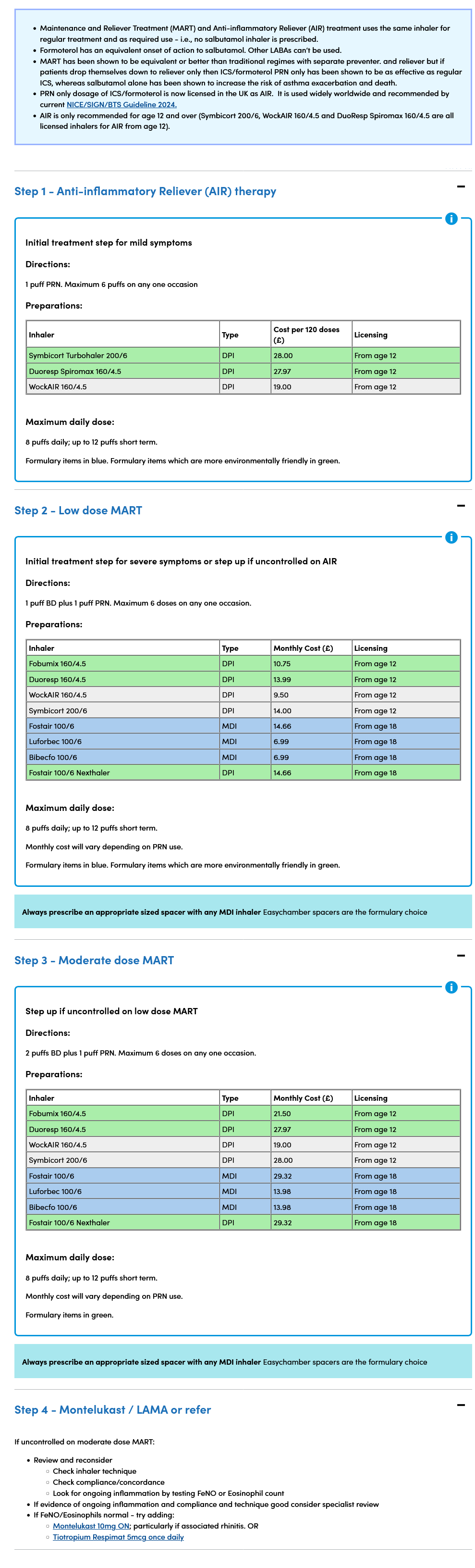
A pragmatic summary of this guidance with practical suggested options has been stated as (2):
Reference:
Create an account to add page annotations
Annotations allow you to add information to this page that would be handy to have on hand during a consultation. E.g. a website or number. This information will always show when you visit this page.