Stages of diabetic nephropathy
Diabetic nephropathy can be classified into normal, microalbuminuria, macroproteinuria and endstage renal disease, according to the amount of albumin excreted. Albumin excretion should be measured on 3-4 samples before persistent microabuminuria is declared to be present as there is often a diurnal variation in excretion of upto 40%. It should also be noted that there is a relationship between the blood pressure and level of proteinuria.
STAGE | Normal | Micro | Macro | End Stage Renal Disease (ESRD) |
albumin excretion (mg/l) | <20 | 20-200 | >200 | >1000 |
blood pressure | 120/75 | 130/85 | 145/95 | 160/100 |
GFR (ml/min) | >110 | >110 | <100 | <30 |
Patients with microalbuminuria often have associated problems of hypertension, left ventricular hypertrophy and insulin resistance.
Patients that develop frank proteinuria are a group that have more problems and appear to have more aggressive disease and particularly have problems with macrovascular disease with an increased mortality.
NICE suggest (1):
- clinicians should use urine albumin:creatinine ratio (ACR) in preference to protein:creatinine ration (PCR) in order to detect proteinuria
- ACR has greater sensitivity than protein:creatinine ratio (PCR) for low levels of proteinuria. For quantification and monitoring of proteinuria, PCR can be used as an alternative. ACR is the recommended method for people with diabetes
- for the initial detection of proteinuria, if the ACR is between 3 mg/mmol and 70 mg/mmol, this should be confirmed by a subsequent early morning sample. If the initial ACR is 70 mg/mmol or more, a repeat sample need not be tested
- regard a confirmed ACR of 3 mg/mmol or more as clinically important proteinuria
- quantify urinary albumin or urinary protein loss for:
- people with diabetes
- people without diabetes with a GFR of less than 60 ml/min/1.73 m^2
- NICE suggested a classification of CKD incorporating GFR and ACR (1)
ACR (albumin creatinine ratio) category | ACR (mg/mmol) |
A1 | <3 |
A2 | 3-30* |
A3 | >30** |
- * Relative to young adult level
- ** Including nephrotic syndrome (ACR usually >220 mg/mmol)
- CKD is classified according to estimated GFR (eGFR) and albumin:creatinine ratio (ACR), using 'G' to denote the GFR category (G1-G5, which have the same GFR thresholds as the CKD stages 1-5 recommended previously) and 'A' for the ACR category (A1-A3), for example:
- a person with an eGFR of 25 ml/min/1.73 m2 and an ACR of 15 mg/mmol has CKD G4A2.
- a person with an eGFR of 50 ml/min/1.73 m2 and an ACR of 35 mg/mmol has CKD G3aA3
- an eGFR of less than 15 ml/min/1.73 m2 (GFR category G5) is referred to as kidney failure
- it is noted that:
- increased ACR is associated with increased risk of adverse outcomes
- decreased GFR is associated with increased risk of adverse outcomes
- increased ACR and decreased GFR in combination multiply the risk of adverse outcomes
This is summarised as (2):
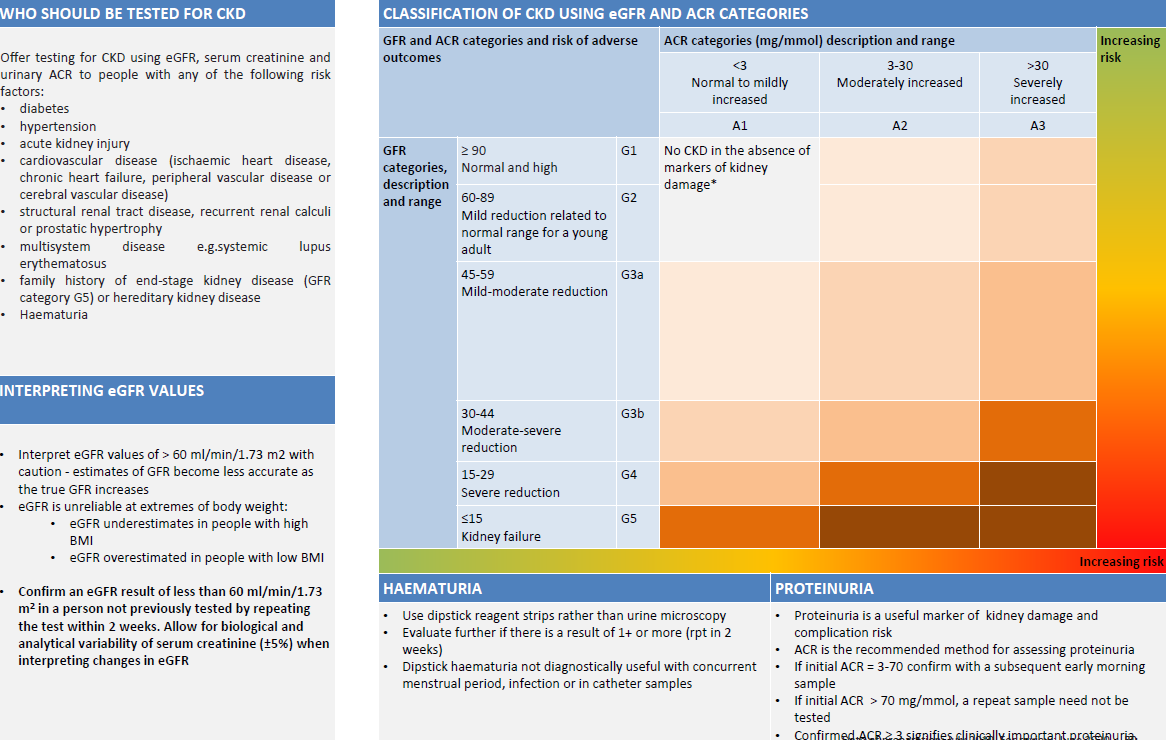
Abbreviations: ACR, albumin:creatinine ratio; CKD, chronic kidney disease
Notes:
- consider using eGFRcystatinC at initial diagnosis to confirm or rule out CKD in people with:
- an eGFRcreatinine of 45-59 ml/min/1.73 m2, sustained for at least 90 days and
- no proteinuria (albumin:creatinine ratio [ACR] less than 3 mg/mmol) or other marker of kidney disease
- do not diagnose CKD in people with:
- an eGFRcreatinine of 45-59 ml/min/1.73 m2 and
- an eGFRcystatinC of more than 60 ml/min/1.73 m2 and
- no other marker of kidney disease
- use of renin-angiotensin system antagonist to people with CKD based on ACR:
- angiotensin-converting enzyme inhibitors (ACE inhibitors)/ angiotensin-II receptor blockers (ARBs) should be offered to non-diabetic people with CKD:
- diabetes and an ACR of 3 mg/mmol or more (ACR category A2 or A3)
- hypertension and an ACR of 30 mg/mmol or more (ACR category A3)
- an ACR of 70 mg/mmol or more (irrespective of hypertension or cardiovascular disease)
- angiotensin-converting enzyme inhibitors (ACE inhibitors)/ angiotensin-II receptor blockers (ARBs) should be offered to non-diabetic people with CKD:
Reference:
- NICE (July 2014). Chronic Kidney Disease - Early identification and management of chronic kidney disease in adults in primary and secondary care
- The North West London Health and Care Partnership. North West London Diabetes Guidelines (Accessed 30/6/2020).
Create an account to add page annotations
Annotations allow you to add information to this page that would be handy to have on hand during a consultation. E.g. a website or number. This information will always show when you visit this page.