Urgent referral for suspected gynaecological cancer
Gynaecological cancers
Symptoms suggestive of Ovarian cancer
- a referral to a gynaecological cancer service using a suspected cancer pathway referral should be made if physical examination identifies ascites and/or a pelvic or abdominal mass (which is not obviously uterine fibroids)
- tests should be carried out in primary care (see below) if a woman, or a trans man or non-binary person with female reproductive organs (especially if they are aged 50 or over) reports having any of the following symptoms on a persistent or frequent basis – particularly more than 12 times per month:
- persistent abdominal distension (often referred to as 'bloating')
- feeling full (early satiety) and/or loss of appetite
- pelvic or abdominal pain
- increased urinary urgency and/or frequency
- consider carrying out tests in primary care (see below) if a woman, or a trans man or non-binary person with female reproductive organs reports unexplained weight loss, fatigue or changes in bowel habit
- any woman, or trans man or non-binary person with female reproductive organs, who is not suspected of having ovarian cancer, should be advised to return to their GP if their symptoms become more frequent or persistent, or both
- carry out appropriate tests for ovarian cancer (see below) in any woman, or trans man or non-binary person with female reproductive organs who is aged 50 or over and who has experienced symptoms within the last 12 months that suggest irritable bowel syndrome (IBS), because IBS rarely presents for the first time at this age
Suggested tests (1):
- for women, and trans men and non-binary people with female reproductive organs who are aged 39 or under with persistent symptoms that suggest ovarian cancer (see above):
- do not use serum CA125 measurement in isolation for decision making (it is not an accurate indicator of ovarian cancer risk in this age group; although the risk of ovarian cancer is low, it remains a clinical concern and is often diagnosed late)
- consider an urgent, direct access ultrasound scan of the abdomen and pelvis
- if the ultrasound scan is normal:
- identify any other potential causes of the symptoms and investigate as appropriate, and
- if no other cause is identified, advise a return to the GP if the symptoms become more frequent or persistent, or both
- for women, and trans men and non-binary people with female reproductive organs who are aged 40 or over with persistent symptoms that suggest ovarian cancer, measure CA125 in primary care
- arrange an urgent, direct access ultrasound scan of the abdomen and pelvis depending on age and serum CA125 according to the thresholds in table below:
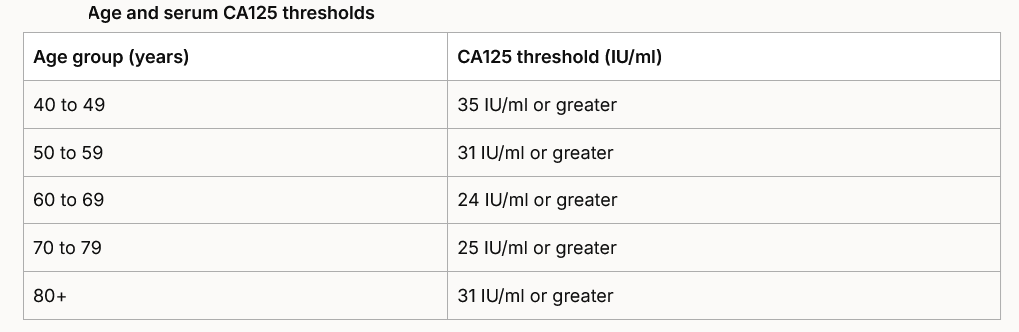
If an ultrasound scan suggests ovarian cancer, make a referral to a gynaecological cancer service using a suspected cancer pathway referral.
If the serum CA125 does not meet the threshold outlined above, or meets the threshold but the ultrasound scan is normal:
- identify any other potential causes of the symptoms and investigate as appropriate, and
- if no other cause is identified, advise a return to the GP if the symptoms become more frequent or persistent, or both
Symptoms suggestive of Endometrial cancer
- refer women using a suspected cancer pathway referral (for an appointment within 2 weeks) for endometrial cancer if they are aged 55 and over with post-menopausal bleeding (unexplained vaginal bleeding more than 12 months after menstruation has stopped because of the menopause)
- consider a suspected cancer pathway referral (for an appointment within 2 weeks) for endometrial cancer in women aged under 55 with post-menopausal bleeding
A direct access ultrasound scan to assess for endometrial cancer should be considered in women aged 55 and over with:
- unexplained symptoms of vaginal discharge who:
- are presenting with these symptoms for the first time or
- have thrombocytosis
- or report haematuria,
- or visible haematuria and:
- low haemoglobin levels or
- thrombocytosis
- or high blood glucose levels
Consider a suspected cancer pathway referral for endometrial cancer in women, and trans men and non-binary people with female reproductive organs who are aged under 55 with unexplained post-menopausal bleeding that cannot be attributed to HRT.
Unscheduled bleeding and HRT
- there is limited evidence for women, and trans men and non-binary people with female reproductive organs who experience unscheduled vaginal bleeding on sequential or continuous HRT
- the British Menopause Society has published guidance on unscheduled bleeding on HRT (British Menopause Society: Management of unscheduled bleeding on HRT)
NICE have provided definitions for (1):
Unexplained post‑menopausal bleeding
- “ ..Vaginal bleeding that cannot be attributed to HRT timing, expected settling-in timing, or any identified benign cause, and therefore requires further assessment to exclude underlying pathology..”
Unscheduled vaginal bleeding on HRT
- “..Vaginal bleeding that occurs after starting or changing an HRT regimen that is expected to be bleed-free (continuous combined HRT), or bleeding that occurs in addition to the planned withdrawal bleed (sequential HRT). It can occur within the first 6 months of starting HRT, or within 3 months of changing a dose or preparation..”
Cervical cancer
- consider a suspected cancer pathway referral (for an appointment within 2 weeks) for women if, on examination, the appearance of their cervix is consistent with cervical cancer
- information regarding urgent referral for post-coital bleeding (2,3)
- the NHS Cancer Screening Programme document "Colposcopy and Programme Management" (3) says:
- women presenting with symptoms of cervical cancer - such as postcoital bleeding (particularly in women over 40 years), intermenstrual bleeding and persistent vaginal discharge - should be referred for gynaecological examination and onward referral for colposcopy if cancer is suspected
- examination should be performed by a gynaecologist experienced in the management of cervical disease (such as a cancer lead gynaecologist)
- they should be seen urgently, within two weeks of referral
- women presenting with symptoms of cervical cancer - such as postcoital bleeding (particularly in women over 40 years), intermenstrual bleeding and persistent vaginal discharge - should be referred for gynaecological examination and onward referral for colposcopy if cancer is suspected
- extracts from the 2019 Scottish referral guidelines are:
- cervical cancer
- majority of cases (80%) are diagnosed on speculum examination and up to 40% are screen detected. Typical symptoms include vaginal discharge, postmenopausal bleeding, postcoital bleeding and persistent intermenstrual bleeding. A cytology test is not required before referral, and a previous negative result is not a reason to delay referral.
- guidelines for urgent referral:
- any woman with clinical features (vaginal discharge, postmenopausal, postcoital and persistent intermenstrual bleeding) and abnormality suggestive of cervical cancer on examination of the cervix
- any woman with clinical features (vaginal discharge, postmenopausal, postcoital and persistent intermenstrual bleeding) and abnormality suggestive of cervical cancer on examination of the cervix
- cervical cancer
- the NHS Cancer Screening Programme document "Colposcopy and Programme Management" (3) says:
Suspected Vulval cancer
- consider a suspected cancer pathway referral (for an appointment within 2 weeks) for vulval cancer in women with an unexplained vulval lump, ulceration or bleeding
Suspected Vaginal cancer
- consider a suspected cancer pathway referral (for an appointment within 2 weeks) for vaginal cancer in women with an unexplained palpable mass in or at the entrance to the vagina
Reference:
- Suspected cancer: recognition and referral. NICE guideline [NG12] Published: 23 June 2015 Last updated: April 15th 2026
- NHS Cancer Screening Programme. Colposcopy and Programme Management. Guidelines for the NHS Cervical Screening Programme. Last updated January 2023
- Scottish Executive Scottish Referral Guidelines for Suspected Cancer. 2019
Related pages
Create an account to add page annotations
Annotations allow you to add information to this page that would be handy to have on hand during a consultation. E.g. a website or number. This information will always show when you visit this page.