Management of infertility
Male factors - loose clothing, abstinence from hot baths, clomiphene, intrauterine or donor insemination.
Ovulatory dysfunction - clomiphene citrate, gonadotrophins, pulsatile GnRH, bromocriptine.
Luteal phase deficiency - progesterone, clomiphene.
Tubal damage - surgery.
Cervical factor - bicarbonate douches, intrauterine insemination.
Endometriosis - laparoscopic ablation may increase fecundity in the short term i.e. the capacity to become pregnant, but not long term fertility rates. Assisted reproduction may be advised especially as it will bypass any peritoneal presence of inhibitory factors to gamete function.
NICE suggest (1):
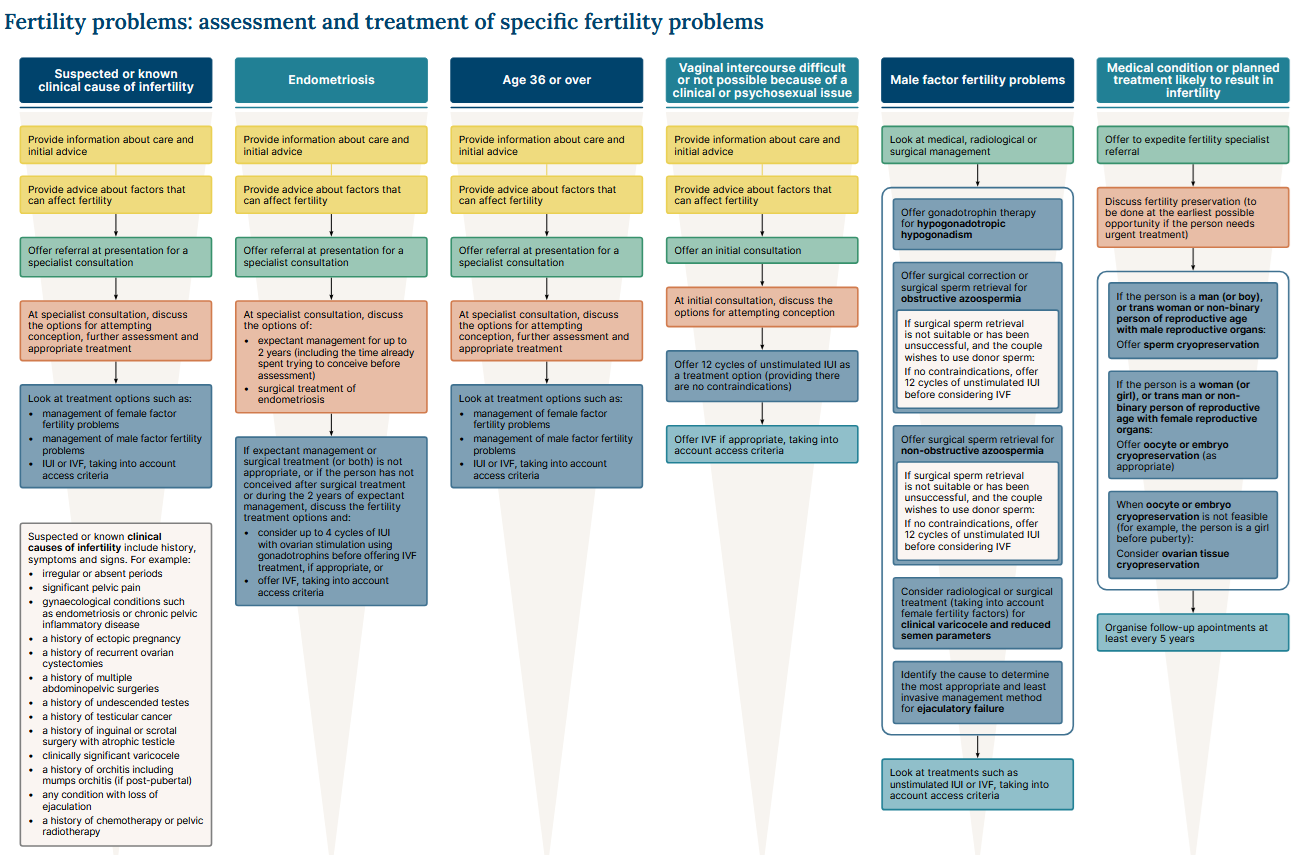
Reference
- NICE. Fertility problems: assessment and treatment. Clinical guideline CG156. Published February 2013, last updated March 2026
Related pages
Create an account to add page annotations
Annotations allow you to add information to this page that would be handy to have on hand during a consultation. E.g. a website or number. This information will always show when you visit this page.