Carpometacarpal osteoarthritis is quite common in postmenopausal women. Heberden's nodes of the finger joints are often also present.
The patient presents with a painful wrist. The pain can be localised to a point distal to the anatomical snuff box. The condition is generally bilateral. There may be swelling or deformity at the base of the thumb metacarpal.
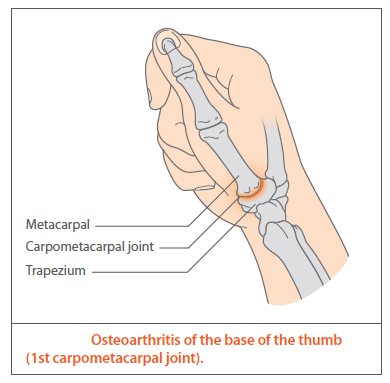
- OA of the base of the thumb, or 1st CMCJ (carpometacarpal joint), should be considered a specific subset of OA
- the ability to oppose thumb and little finger allows for fine coordinated movement of the hand
- arthritis of the thumb is often painful and debilitating. OA thumb is more common in females but may affect males
- more commonly seen in patients older than 50 years
- base of the thumb becomes squared in shape (if in doubt compare with your own thumb!) and may be red, swollen and painful. There may be wasting of the muscles of the thenar eminence (always look out for co-existing carpal tunnel syndrome)
Management:
- X-rays will confirm the diagnosis of OA of the 1st CMCJ and may also show arthritis in neighbouring joints
- analgesia is often prescribed in OA thumb but is seldom effective due to the constant stresses placed upon the thumb in daily activity
- localised topical non-steroidal anti-inflammatory drug (NSAID) gel may have a mild analgesic effect without systemic side-effects
- static splinting maintains optimal joint alignment and reduces the forces that may lead to further joint deterioration or deformity
- resting thumb splints (spicas) can offer significant relief; however, where there is severe squaring of the base of thumb bespoke splints will be required to accommodate the deformity
- corticosteroid injections may offer pain relief for up to 6 months and can be repeated as necessary
- hydrocortisone should be used and care must be taken to avoid local vascular structures
- ultrasound-guided injections may be performed where blind injections have failed.
- surgery should be considered for all patients who have failed to respond to the above measures or where x-rays have shown bone-on-bone arthritis
- there are several surgical procedures available, the most common being excision arthroplasty of the trapezium
Reference:
- (1) Arthritis Research UK (April 2013). The upper limb in primary care. Part 2: Wrist, hand. Hands On 2(7)
Create an account to add page annotations
Annotations allow you to add information to this page that would be handy to have on hand during a consultation. E.g. a website or number. This information will always show when you visit this page.