Management of chronic asthma in adults
Last reviewed dd mmm yyyy. Last edited dd mmm yyyy
The aim of asthma management is control of the disease. Complete control is defined as
- no daytime symptoms
- no night-time awakening due to asthma
- no need for rescue medication
- no asthma attacks
- no limitations on activity including exercise
- normal lung function (in practical terms FEV1 and/or PEF >80% predicted or best)
- minimal side effects from medication.
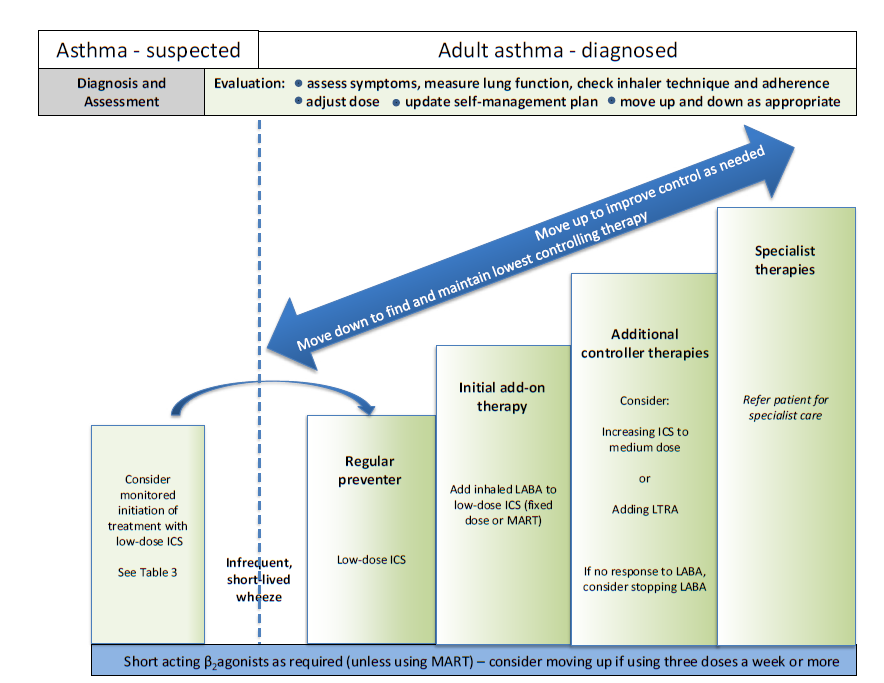
Approach to Management:
- 1. Start treatment at the level most appropriate to initial severity.
- 2. Achieve early control.
- 3. Maintain control by:
- increasing treatment as necessary
- decreasing treatment when control is good
Decreasing Treatment:
- Regular review of patients as treatment is decreased is important. When deciding which drug to decrease first and at what rate, the severity of asthma, the side effects of the treatment, time on current dose, the beneficial effect achieved, and the patient’s preference should all be taken into account
- Patients should be maintained at the lowest possible dose of inhaled corticosteroid. Reduction in inhaled corticosteroid dose should be slow as patients deteriorate at different rates. Reductions should be considered every three months, decreasing the dose by approximately 25-50% each time
Pharmacological Management in adults
Step-up treatment if ventolin is needed more than 3 times a week.
Exercise Induced Asthma:
- For most patients, exercise-induced asthma is an expression of poorly-controlled asthma and regular treatment including inhaled corticosteroids should be reviewed
- If exercise is a specific problem in patients taking inhaled corticosteroids who are otherwise well controlled, consider adding one of the following therapies:
- leukotriene receptor antagonists
- long-acting beta 2 agonists
- sodium cromoglicate or nedocromil sodium
- oral beta 2 agonists
- theophyllines
- If exercise is a specific problem in patients taking inhaled corticosteroids who are otherwise well controlled, consider adding one of the following therapies:
- Immediately prior to exercise, inhaled short-acting beta2 agonists are the drug of choice
Maintenance and Reliever Therapy (MART)
- when prescribed a combination inhaler to be used as both your preventer and your reliever as part of a specific treatment regime.
Reference:
- SIGN (July 2019). British Guideline on the management of asthma (SIGN158).
Create an account to add page annotations
Annotations allow you to add information to this page that would be handy to have on hand during a consultation. E.g. a website or number. This information will always show when you visit this page.