Management of chronic angina
A patient with newly diagnosed angina should be referred for formal cardiology assessment. Specialist advice may also be sought if there is a recurrence or worsening of angina symptoms. Emergency referral is required if unstable angina is suspected.
General management:
- patient should be advised about
- discontinuing the activity which provoked the angina and rest
- use of sublingual nitrate for acute relief of symptoms
- patients need to seek medical advice if angina persists for 10-20 min after resting and/or is not relieved by sublingual nitrate
- lifestyle measures
- increase physical activity without excessive exertion
- stopping smoking
- follow a 'Mediterranean' diet which includes mainly vegetables, fruits, fish and poultry
- weight control
- consumption of fish oils rich in omega-3 fatty acids (1)
- managing other cormorbidties which increase cardiovascular events accordingly e.g. - hypertension, diabetes mellitus, anaemia, hyperthyroidism, hyperlipidaemia
- sexual intercourse may precipitate angina, taking glyceryl trinitrate before intercourse may help prevent anginal attacks (1)
- due to the risk of hypotension Phosphodiesterase type 5 inhibitors (e.g., sildenafil, vardenafil, and tadalafil) should not be given to patients taking long acting nitrates
- the use of nitrates/nicorandil with phosphodiesterase inhibitors is described in the linked item below
- due to the risk of hypotension Phosphodiesterase type 5 inhibitors (e.g., sildenafil, vardenafil, and tadalafil) should not be given to patients taking long acting nitrates
- work
- most people with angina go back and continue their work as before but people doing heavy manual work may have to alter their profession
- in driving profession, patients should consult the Driver and Vehicle Licensing Agency
Pharmacological management
- for symptomatic relief
- a short acting sublingual glyceryl trinitrate - should be used for symptomatic relief of anginal attacks and for "situational prophylaxis" e.g. - before carrying out activities which may precipitate anginal attacks
- NICE (1) state that:
- offer a short-acting nitrate for preventing and treating episodes of angina.
- advise people with stable angina:
- to use it immediately before any planned exercise or exertion
- when a short-acting nitrate is being used to treat episodes of angina, advise people:
- to repeat the dose after 5 minutes if the pain has not gone
- to call an emergency ambulance if the pain has not gone 5 minutes after taking a second dose
- advise people with stable angina:
- offer a short-acting nitrate for preventing and treating episodes of angina.
- drugs for secondary prevention of cardiovascular disease
- consider aspirin 75 mg daily for people with stable angina, taking into account the risk of bleeding and comorbidities
- consider angiotensin-converting enzyme (ACE) inhibitors for people with stable angina and diabetes
- offer or continue ACE inhibitors for other conditions, in line with relevant NICE guidance
- offer statin treatment in consideration of NICE guidance
- offer treatment for high blood pressure in line with NICE guidance
- anti-anginal drug treatment
- principles
- optimal drug treatment consists of one or two anti-anginal drugs as necessary plus drugs for secondary prevention of cardiovascular disease
- review the person's response to treatment, including any side effects, 2-4 weeks after starting or changing drug treatment
- titrate the drug dosage against the person's symptoms up to the maximum tolerable dosage
- drugs for treating stable angina
- offer either a beta blocker or a calcium channel blocker as first-line treatment for stable angina. The decision on which drug to use is based on comorbidities, contraindications and the person's preference
- if the person cannot tolerate the beta blocker or calcium channel blocker, consider switching to the other option (calcium channel blocker or beta blocker)
- if the person's symptoms are not satisfactorily controlled on a beta blocker or a calcium channel blocker, consider either switching to the other option or using a combination of the two
- do not routinely offer anti-anginal drugs other than beta blockers or calcium channel blockers as first-line treatment for stable angina
- if the person cannot tolerate beta blockers and calcium channel blockers or both are contraindicated, consider monotherapy with one of the following drugs:
- a long-acting nitrate or
- ivabradine or
- nicorandil or
- ranolazine
- for people on beta blocker or calcium channel blocker monotherapy whose symptoms are not controlled and the other option (calcium channel blocker or beta blocker) is contraindicated or not tolerated, consider one of the following as an additional drug:
- a long-acting nitrate or
- ivabradine (a sinus node inhibitor) or
- nicorandil or
- ranolazine
- consider adding a third anti-anginal drug only when:
- the person's symptoms are not satisfactorily controlled with two anti-anginal drugs and
- the person is waiting for revascularisation or revascularisation is not considered appropriate or acceptable.
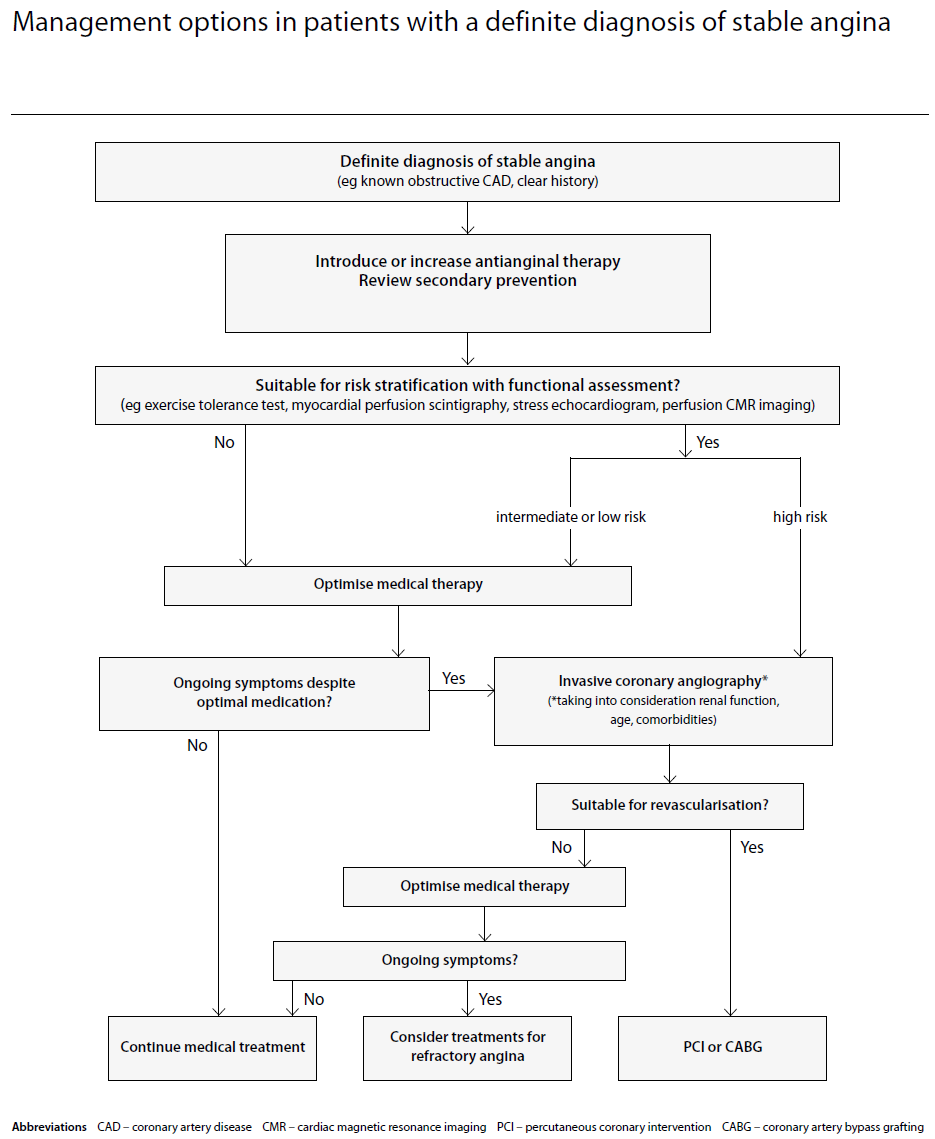
- principles
- people with stable angina whose symptoms are not satisfactorily controlled with optimal medical treatment
- consider revascularisation (coronary artery bypass graft [CABG] or percutaneous coronary intervention [PCI]) for people with stable angina whose symptoms are not satisfactorily controlled with optimal medical treatment
- offer coronary angiography to guide treatment strategy for people with stable angina whose symptoms are not satisfactorily controlled with optimal medical treatment. Additional non-invasive or invasive functional testing may be required to evaluate angiographic findings and guide treatment decisions
- offer CABG to people with stable angina and suitable coronary anatomy when:
- their symptoms are not satisfactorily controlled with optimal medical treatment and
- revascularisation is considered appropriate and
- PCI is not appropriate
- offer PCI to people with stable angina and suitable coronary anatomy when:
- their symptoms are not satisfactorily controlled with optimal medical treatment and
- revascularisation is considered appropriate and
- CABG is not appropriate
- when either procedure would be appropriate, explain to the person the risks and benefits of PCI and CABG for people with anatomically less complex disease whose symptoms are not satisfactorily controlled with optimal medical treatment. If the person does not express a preference, take account of the evidence that suggests that PCI may be the more cost-effective procedure in selecting the course of treatment
- When either procedure would be appropriate, take into account the potential survival advantage of CABG over PCI for people with multivessel disease whose symptoms are not satisfactorily controlled with optimal medical treatment and who:
- have diabetes or
- are over 65 years or
- have anatomically complex three-vessel disease, with or without involvement of the left main stem
- when either revascularisation procedure is appropriate, explain to the person:
- the main purpose of revascularisation is to improve the symptoms of stable angina
- CABG and PCI are effective in relieving symptoms
- repeat revascularisation may be necessary after either CABG or PCI and the rate is lower after CABG
- stroke is uncommon after either CABG or PCI, and the incidence is similar between the two procedures
- there is a potential survival advantage with CABG for some people with multivessel disease
- offer coronary angiography to guide treatment strategy for people with stable angina whose symptoms are not satisfactorily controlled with optimal medical treatment. Additional non-invasive or invasive functional testing may be required to evaluate angiographic findings and guide treatment decisions
- consider revascularisation (coronary artery bypass graft [CABG] or percutaneous coronary intervention [PCI]) for people with stable angina whose symptoms are not satisfactorily controlled with optimal medical treatment
SIGN suggest that (3):
patients whose symptoms are not controlled on maximum therapeutic doses of two drugs should be considered for referral to a cardiologist
- patients with Prinzmetal (vasospastic) angina should be treated with a dihydropyridine derivative calcium channel blocker, eg (amlodipine, nifedipine)
Notes:
- one must also consider co-morbidity:
- renal disease
- peripheral vascular disease
- aortic stenosis
- asthma
- when combining ivabradine with a calcium channel blocker, use a dihydropyridine calcium channel blocker, for example, slow release nifedipine, amlodipine, or felodipine (2)
- beta blockers
- beta-1 selective agents are favored e.g. - metoprolol, atenolol and bisoprolol (1)
- beta-1 selective agents are favored e.g. - metoprolol, atenolol and bisoprolol (1)
- combination therapy - when anginal symptoms are not adequately controlled, certain drug combinations may be used
- including a CCB to a beta blocker - dihydropyridines are preferred
- verapamil acts primarily to reduce the force of myocardial contraction and to limit heart rate
- extreme caution is required if combining verapamil with a beta-blocker - in general this combination should be avoided
- diltiazem - has properties intermediate between verapamil and the dihydropyridines but again the combination of diltiazem with a beta-blocker is generally avoided
- verapamil acts primarily to reduce the force of myocardial contraction and to limit heart rate
- including a CCB to a beta blocker - dihydropyridines are preferred
- to improve prognosis
- all patients with stable angina should receive long term (1,3)
- antithrombotic drugs - aspirin (75mg per day)
- lipid lowering agents (3)
- BP control - BP < 145/85 mmHg
- angiotensin-converting enzyme (ACE) inhibitor should be considered for all patients with stable angina (3)
- if there are no contraindications an ACE inhibitor should be given for angina patients with ventricular dysfunction, hypertension or diabetes and should be considered in patients with other high-risk features (1)
- all patients with stable angina should receive long term (1,3)
Reference:
- 1. Fox K et al. Guidelines on the management of stable angina pectoris: executive summary. European Heart Journal 2006;27(11):1341-1381
- 2.NICE (August 2016). Stable angina.
- 3. SIGN (April 2018). Management of Stable Angina.
Related pages
- Coronary angioplasty
- Coronary artery bypass grafting (off pump and via cardiopulmonary bypass)
- Indications for coronary angioplasty or surgery
- Aspirin in angina
- Beta-blockers
- Cholesterol-lowering therapy
- Nicorandil
- Calcium channel blockers in angina
- Ivabradine
- Sildenafil and nitrates
- NICE guidance - rivaroxaban for preventing atherothrombotic events in people with coronary or peripheral artery disease
Create an account to add page annotations
Add information to this page that would be handy to have on hand during a consultation, such as a web address or phone number. This information will always be displayed when you visit this page