Management of chronic asthma in children under 5
NICE state (1):
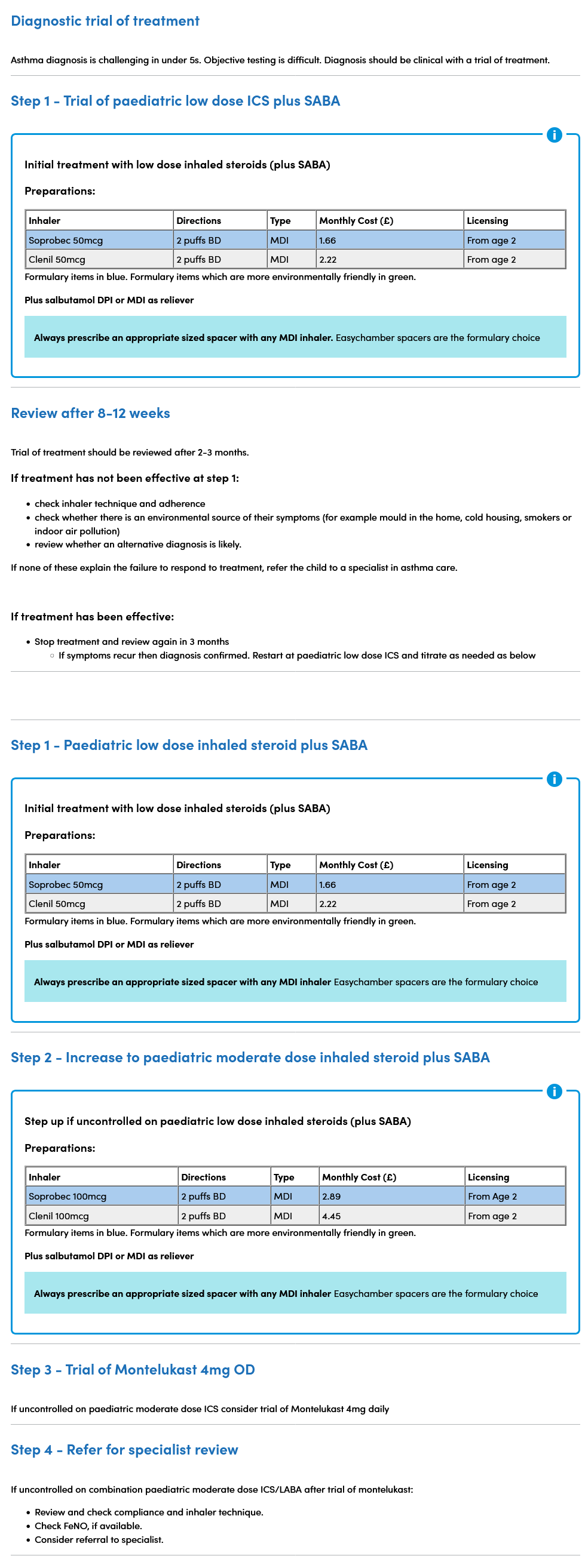
- an 8 to12 week trial of twice-daily paediatric low-dose inhaled corticosteroid (ICS) as maintenance therapy (with a short-acting beta2 agonist [SABA] for reliever therapy) should be considered in children under 5 with suspected asthma and:
- symptoms at presentation that indicate the need for maintenance therapy (for example, interval symptoms in children with another atopic disorder, or
- severe acute episodes of difficulty breathing and wheeze (for example, requiring hospital admission, or needing 2 or more courses of oral corticosteroids)
- if symptoms do not resolve during the trial period, take the following sequential steps:
- check inhaler technique and adherence
- check whether there is an environmental source of their symptoms (for example mould in the home, cold housing, smokers or indoor air pollution)
- review whether an alternative diagnosis is likely
- if none of these explain the failure to respond to treatment, refer the child to a specialist in asthma care (https://www.nice.org.uk/guidance/ng245/chapter/recommendations#specialist-in-asthma-care)
- consider stopping ICS and SABA treatment after 8 to 12 weeks if symptoms are resolved. Review the symptoms after a further 3 months
- if symptoms resolve during the trial period, but then:
- symptoms recur by the 3-month review, or
- the child has an acute episode requiring systemic corticosteroids or hospitalisation, restart regular ICS (begin at a paediatric low dose and titrate up to a paediatric moderate dose if needed) with SABA as needed and consider a further trial without treatment after reviewing the child within 12 months
- if suspected asthma is uncontrolled in children under 5 on a paediatric moderate dose of ICS as maintenance therapy (with SABA as needed), consider a leukotriene receptor antagonist (LTRA) in addition to the ICS
- the LTRA should be given for a trial period of 8 to 12 weeks (unless there are side effects), then stop it if it is ineffective
If suspected asthma is uncontrolled in children under 5 on a paediatric moderate dose of ICS as maintenance therapy and a trial of an LTRA has been unsuccessful or not tolerated, stop the LTRA and refer the child to a specialist in asthma care for further investigation and management.
Decreasing maintenance therapy Principles:
When decreasing maintenance therapy:
- stop or reduce dose of medicines in an order that takes into account the clinical effectiveness when introduced, side effects and the person's preference.
- allow at least 8 to 12 weeks before considering a further treatment reduction
- if considering step-down treatment for people aged 12 and over who are using low-dose maintenance inhaled corticosteroid (ICS) plus a short-acting beta2 agonist (SABA) as needed or low-dose MART, step down to low-dose ICS/formoterol combination inhaler as needed (as-needed AIR therapy
A pragmatic summary of this guidance with practical suggested options has been stated as (2):
Reference:
Create an account to add page annotations
Add information to this page that would be handy to have on hand during a consultation, such as a web address or phone number. This information will always be displayed when you visit this page