Gallbladder polyp
- Gallbladder polyps
- are found in up to 4% of patients on ultrasound scan (1)
- the term polyp encompasses a heterogeneous group of abnormalities, including true polyps, polypoid tumours such as adenomas, and pseudotumours, which may be either inflammatory polyps or epithelium-covered aggregates of lipid-laden macrophages, also termed cholesterol polyps
- although gallbladder cancers can present as polypoid lesions, the relation between gallbladder polyps and cancer is controversial
- majority of polypoid lesions of the gallbladder (PLG) are benign (2)
- a small minority (5%) of PLG are ‘true’ adenomatous gallbladder polyps (GBP) with malignant potential (2)
- is estimated that 3–8% of GBP are malignant and that of adenomatous polyps measuring > 10 mm, about 50% will harbor cancerous cells. In the UK, approximately 50 000 laparoscopic cholecystectomies (LCs) are performed each year, of which 800–4000 are estimated to be for GBP
- is estimated that 3–8% of GBP are malignant and that of adenomatous polyps measuring > 10 mm, about 50% will harbor cancerous cells. In the UK, approximately 50 000 laparoscopic cholecystectomies (LCs) are performed each year, of which 800–4000 are estimated to be for GBP
- gallbladder polyps are generally thought to be asymptomatic and indeed are commonly described as incidental findings on radiological imaging (2)
- a smaller proportion of patients may be symptomatic with typical biliary symptoms, but GBP are often associated with gallstones, which makes it difficult to establish whether they are responsible for the reported symptomatology
- a smaller proportion of patients may be symptomatic with typical biliary symptoms, but GBP are often associated with gallstones, which makes it difficult to establish whether they are responsible for the reported symptomatology
- polyps and cancer
- gallbladder cancer (GBC) is a relatively rare neoplasm in the UK, but cumulative 5-year survival rates are only 5–10% (2)
- some experts consider there is a polyp-to-cancer sequence in which some adenomas progress to adenocarcinoma
- others believe most gallbladder carcinomas arise in situ from flat, dysplastic epithelium
- some clues to the nature of the polyp can be gleaned from ultrasonographic appearances
- cholesterol polyps, which are the commonest polypoid lesions and have no malignant potential, are characteristically small, multiple, and hyperechoic on ultrasound because of their cholesterol content
- the size of the polyp is also suggestive of the underlying pathology
- study evidence found that:
- of 32 benign polyps, 30 were under 10 mm in diameter, whereas seven of eight malignant lesions were larger, and of these five had been correctly diagnosed preoperatively on the basis of size or ultrasonographic appearance (3)
- study evidence found that:
- malignant polyps tend to be single and larger, and to occur in older patients
- age is another risk factor. Several studies demonstrated that age older than 50 to 60 years is associated with a higher risk for malignant polyps (2)
- polyps 10 to 20 mm in diameter should be regarded as possibly malignant, laparoscopic cholecystectomy is recommended according to the size criteria
- endoscopic ultrasound (EUS) and gallbladder polyps
- presence of hypoechoic foci on EUS is a strong predictive factor for neoplastic polyps (4)
- at present, EUS is considered to be superior to conventional ultrasonography (US) for imaging the gallbladder. With much higher ultrasound frequencies (7.5 to 12 mHz versus 2 to 5 mHz), EUS can readily image the layer structure of gallbladder wall and provide high-resolution images of small lesions
- hypoechoic foci in central portion of gallbladder polyp is thought to play an important role in determining the treatment strategy and avoiding unnecessary resection for small non-neoplastic gallbladder polyp (4)
- at present, EUS is considered to be superior to conventional ultrasonography (US) for imaging the gallbladder. With much higher ultrasound frequencies (7.5 to 12 mHz versus 2 to 5 mHz), EUS can readily image the layer structure of gallbladder wall and provide high-resolution images of small lesions
- presence of hypoechoic foci on EUS is a strong predictive factor for neoplastic polyps (4)
A suggested algorithm for management of gallbladder polyps is presented (2):
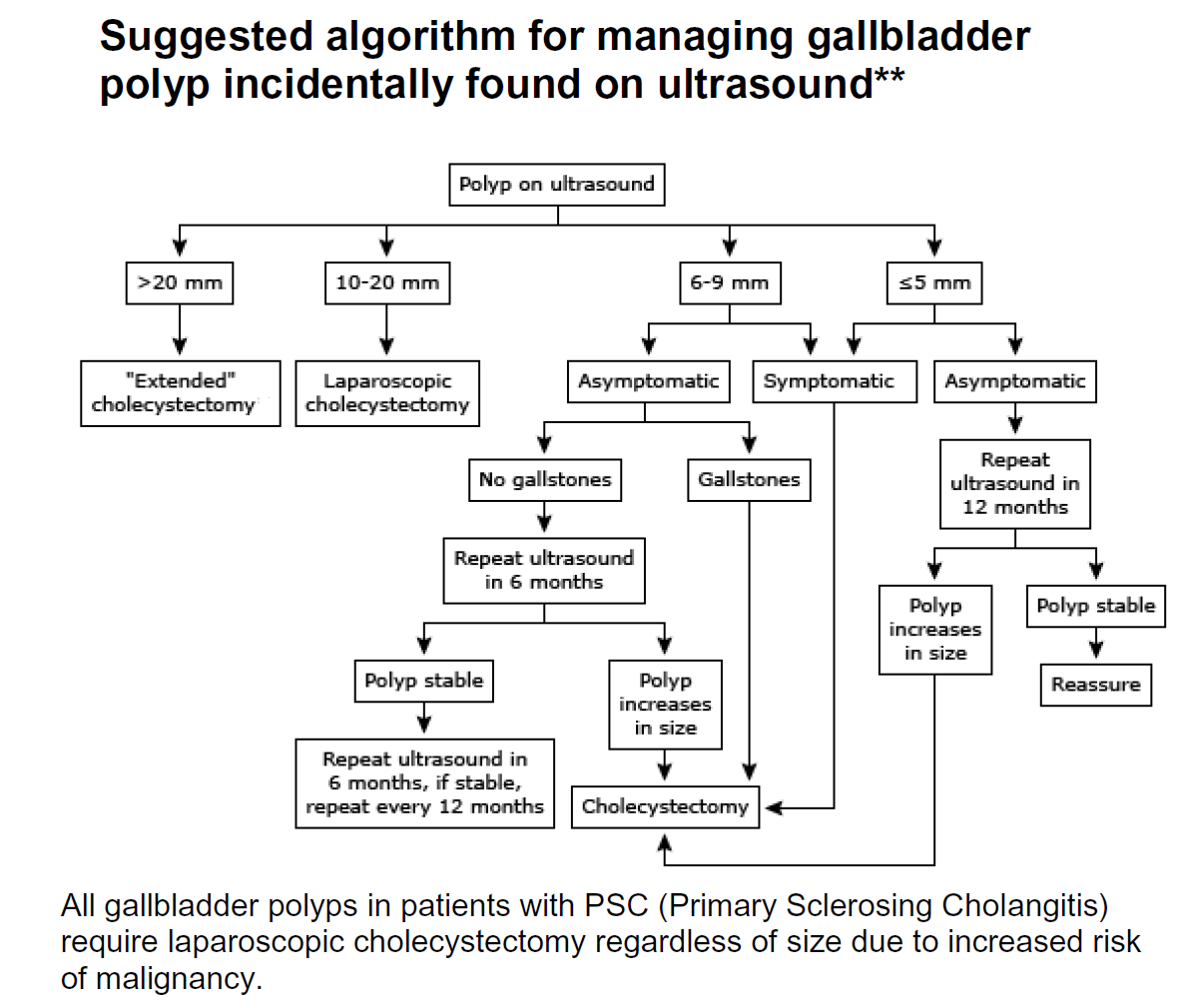
** guidance suggests discussion of polyps >=10mm with a specialist Hepatobiliary centre
Reference:
- Boulton RA, Adams DH. Gallbladder polyps: when to wait and when to act., Lancet 1997;349: 817.
- NHS West Mids (April 2020). West Midlands Cancer Alliance Hepatobiliary Gallbladder Polyps Management Guidelines
- Koga A et al. Polypoid lesions of the gallbladder: diagnosis and indications for surgery. Br J Surg 1992; 79: 227-29.
- Hee JH et al. Hypoechoic foci on EUS are simple and strong predictive factors for neoplastic gallbladder polyps. Gastrointestinal Endoscopy 2009; 69 (7): 1244-1250.
Related pages
Create an account to add page annotations
Add information to this page that would be handy to have on hand during a consultation, such as a web address or phone number. This information will always be displayed when you visit this page