Cardiac failure
Heart failure is a complex clinical syndrome of symptoms and signs that suggest the efficiency of the heart as a pump is impaired (1):
- when this affects mainly the left ventricle, it can be due to either weakness of contraction or impaired relaxation of the left ventricle
- other problems affecting the right ventricle, the heart valves, the pulmonary circulation or the pericardium can lead to the development of heart failure
- almost 1 million people in the UK are currently diagnosed with heart failure, with 200,000 new cases each year
- average age at diagnosis is 76 years. Increases in life expectancy, including for people with ischaemic heart disease and hypertension, has increased the incidence of heart failure
- increased prevalence of obesity is another contributor to the rising incidence and prevalence of heart failure
Heart failure (HF) is a syndrome and not a single pathological process in which there is impairment of the heart as a pump supporting physiological circulation (1). Patients with heart failure will have the following features:
- symptoms typical of heart failure e.g. - breathlessness and exhaustion at rest or with less than the normal degree of exertion, fatigue and
- signs of fluid retention e.g. - pleural effusion, increased JVP, peripheral oedema and
- objective evidence of an abnormality of the structure or function of the heart at rest e.g. - cardiac murmurs, third heart sound (3)
The functional reserve of the heart is grossly reduced and there are associated changes in many organ systems.
Heart failure may be described as acute or chronic:
- acute heart failure - a rapid onset or change in the following signs and symptoms:
- dyspnoea
- oedema, either pulmonary or peripheral
- organ underperfusion
- tachycardia
- chronic heart failure may be more insidious:
- chronic exercise limitation
Due to the confusion in the rate of onset and duration of symptoms in acute and chronic HF, the European Society of Cardiology suggested that HF could more accurately be described as new onset, transient, or chronic (2).
Classification by Left Ventricular Ejection Fraction (LVEF)
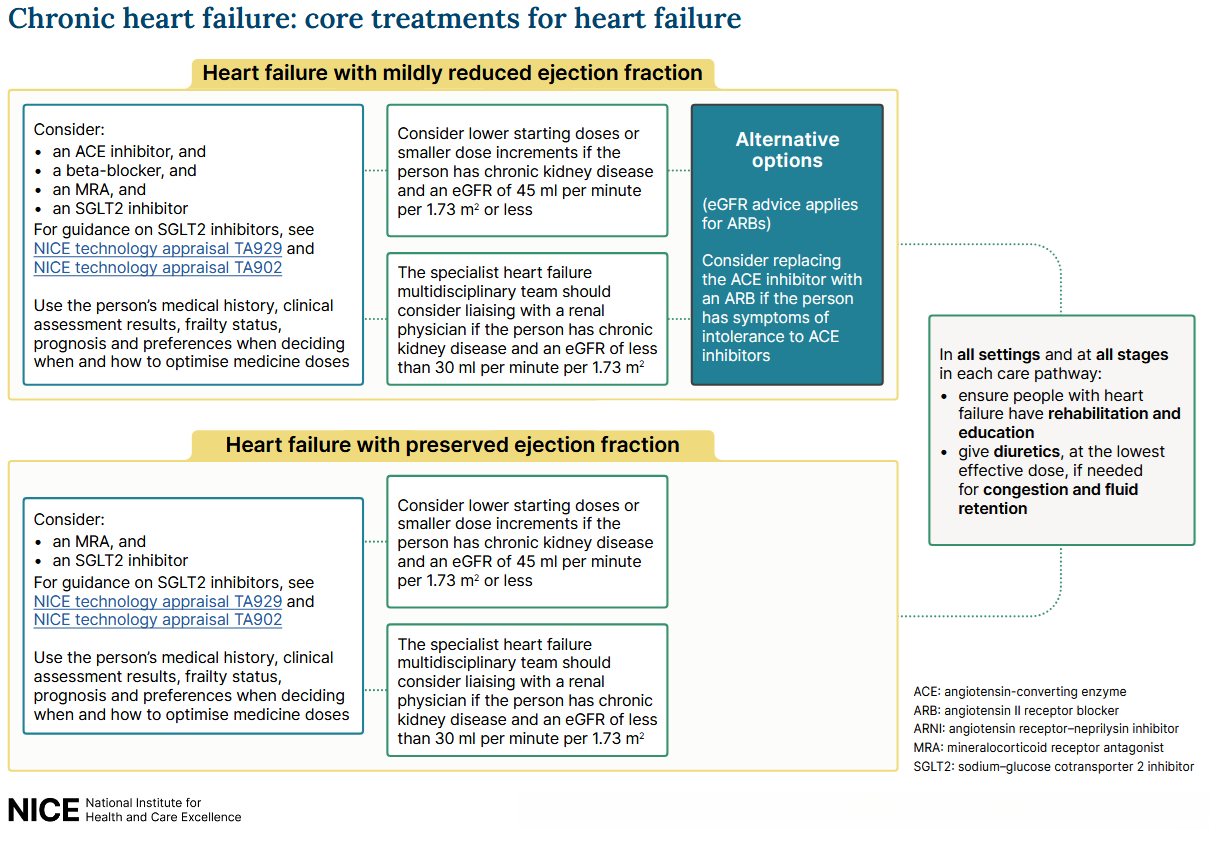
- HF with preserved ejection fraction (HFpEF): an LVEF of ≥50%, formerly known as diastolic heart failure
- HF with mildly reduced ejection fraction (HFmrEF): an LVEF of 41% to 49%.
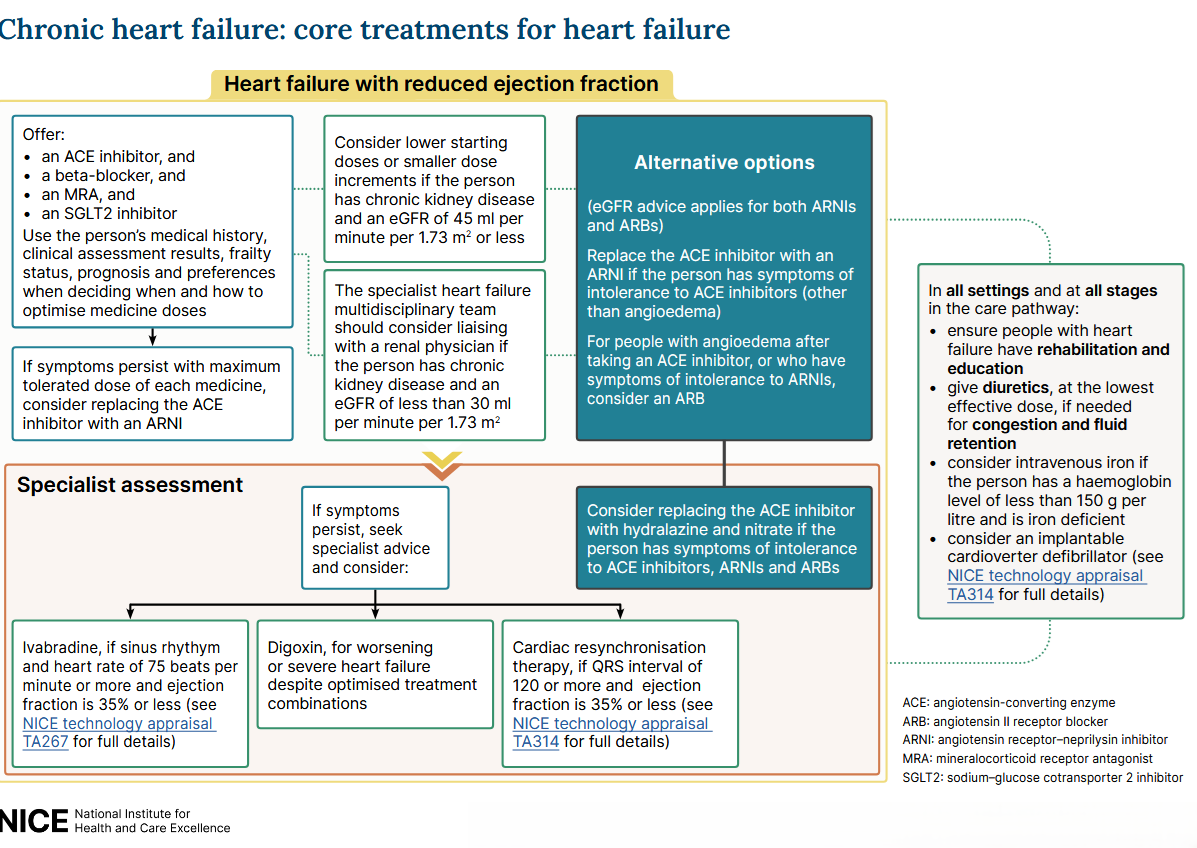
- HF with reduced ejection fraction (HFrEF): an LVEF of ≤40%.
- HF with improved ejection fraction (HFimpEF): defined by a baseline LVEF ≤40%, an increase of ≥10% from the baseline, and a subsequent measurement of LVEF >40%
NICE have suggested management of chronic heart failure based on the LVEF classification above (1):
Fluid restriction and heart failure
- limiting fluid intake may have no benefit for patients with chronic heart failure, according to findings from the FRESH-UP study (3)
Heart failure in women (4)
- a study (n=3,692,157) found oral contraceptive use & menopausal hormone therapy were linked to lower heart failure (HF) risk, and lower mortality among women with HF, whereas later menarche, earlier menopause & shorter reproductive period with higher HF risk
Reference:
- NICE. Chronic heart failure in adults: diagnosis and management. NICE guideline NG106. Published September 2018, last updated September 2025
- European Society of Cardiology. Clinical Practice Guidelines. 2023 Focused Update of the 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure.
- Beckers-Wesche F et al. Liberal fluid intake versus fluid restriction in chronic heart failure: a randomized clinical trial. Nat Med. 2025 Mar 30.
- Kim L et al. Reproductive history, hormonal exposure, and risk of heart failure in postmenopausal women: a Korean nationwide study, European Heart Journal, 2026;, ehag380.
Related pages
- Classification
- Epidemiology
- Pathophysiology
- Risk factors
- Clinical features
- Investigations
- Diagnosis of heart failure (left ventricular dysfunction) in primary care
- Differential diagnosis
- Management of heart failure
- Complications
- Prognosis
- NICE guidance - chronic heart failure (CHF)
- Referral criteria from primary care - chronic heart failure (CHF)
- Congestive cardiac failure (and fitness to fly)
- Driving and cardiovascular disease (CVD)
- Brain type ( B type BNP ) natriuretic peptide in the detection of congestive heart failure
- Brain type ( B type BNP ) natriuretic peptide in the detection of acute heart failure
- SGLT2 inhibitors and heart failure
- Sacubutril
Create an account to add page annotations
Add information to this page that would be handy to have on hand during a consultation, such as a web address or phone number. This information will always be displayed when you visit this page