Aspiration or injection of the knee joint
Last reviewed dd mmm yyyy. Last edited dd mmm yyyy
Aspiration and Injection of the knee Joint
Based on contributions from Dr Elspeth Wise and Dr Alan Walker on behalf of the Primary Care Rheumatology and Musculoskeletal Medicine Society
Aspirating and injecting the knee joint can be extremely useful in the diagnosis and management of knee problems. There are a limited number of injections that can be performed at the knee joint. These include:
- Knee joint:
- lateral approach
- medial approach
- anterior approach
- suprapatella pouch (if an effusion is present)
- lateral approach
- anserine bursa injection
- pre-patella bursitis injection
The choice of site and approach depends on the experience of the clinician, the nature of the symptoms and the precise diagnosis. A good knowledge of anatomy is essential and only clinicians experienced in these procedures should be performing them.
Injection of the knee joint
The knee joint may be injected for conditions such as osteoarthritis, inflammatory arthritis, crystal arthropathies (e.g. gout) and in the presence of Baker's cysts.
Aspiration of the joint can be an extremely useful tool to aid diagnosis and can also be therapeutic.
The knee joint can be accessed via a medial, lateral or anterior approach.
The medial and lateral approaches are classically performed with the patient lying flat whereas the anterior approach can be performed with the patient sitting on a couch
- preferences vary as to which approach is used and often depends on the operator's experience
- if a significant effusion is present, it is possible to aspirate and inject into the supra-patella pouch directly
- dose of steroid used also varies between different preparations and guidance is available in reputable textbooks/guidelines
- local anaesthetic is also often used mixed in with the steroid as a way of increasing the volume of the injection
Appropriate informed consent, aseptic technique and aftercare with rest of the knee for 24-48 hours should be applied in all cases
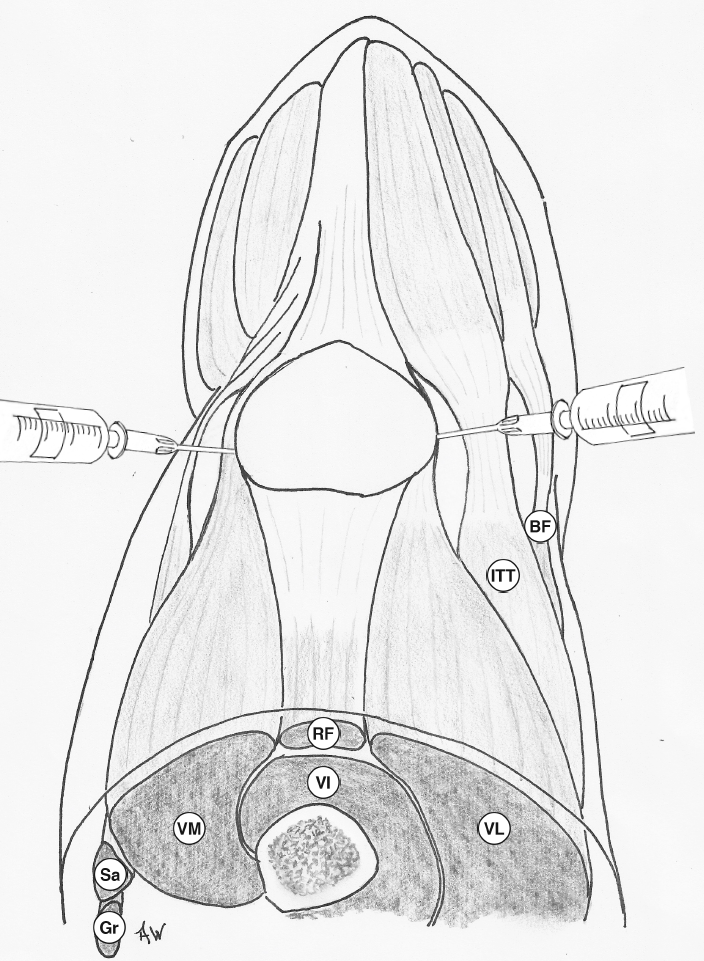
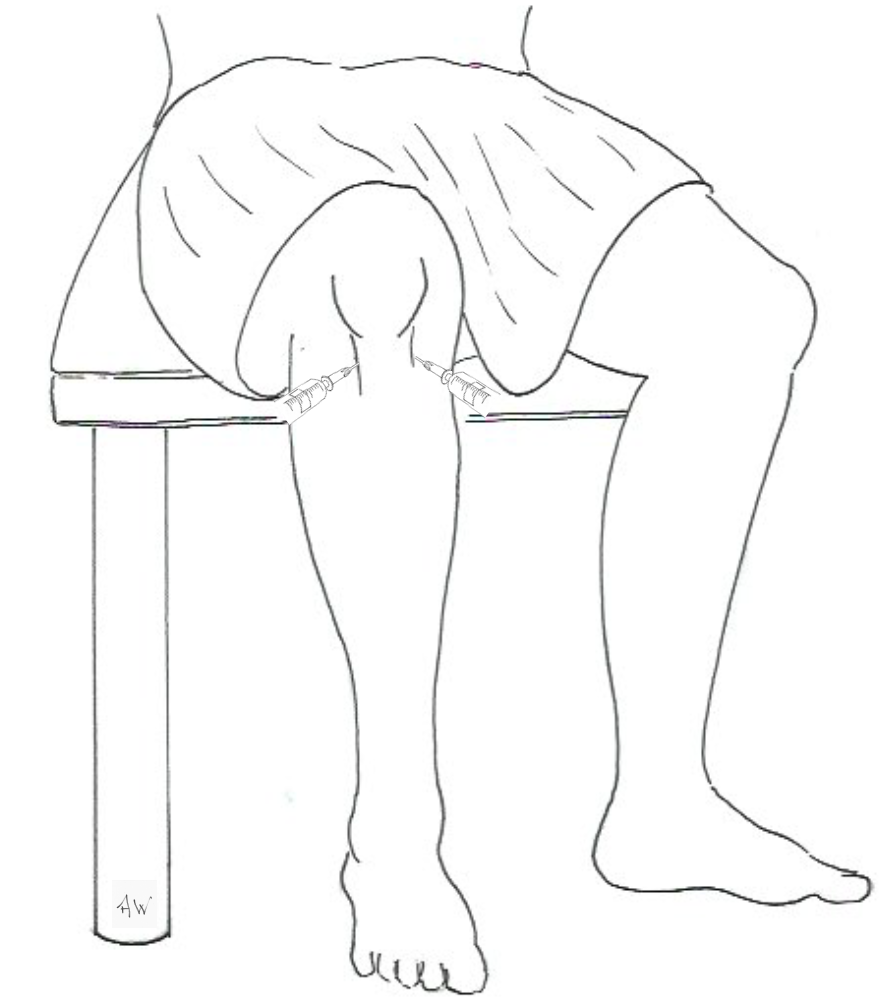
Sites of injection for medial and lateral injection of the knee joint - surface anatomy:
Medial and Lateral injection sites of the knee joint - anatomical diagram:
Medial and Lateral Injection - Needle tip site:

Anterior approach to injection of knee joint:
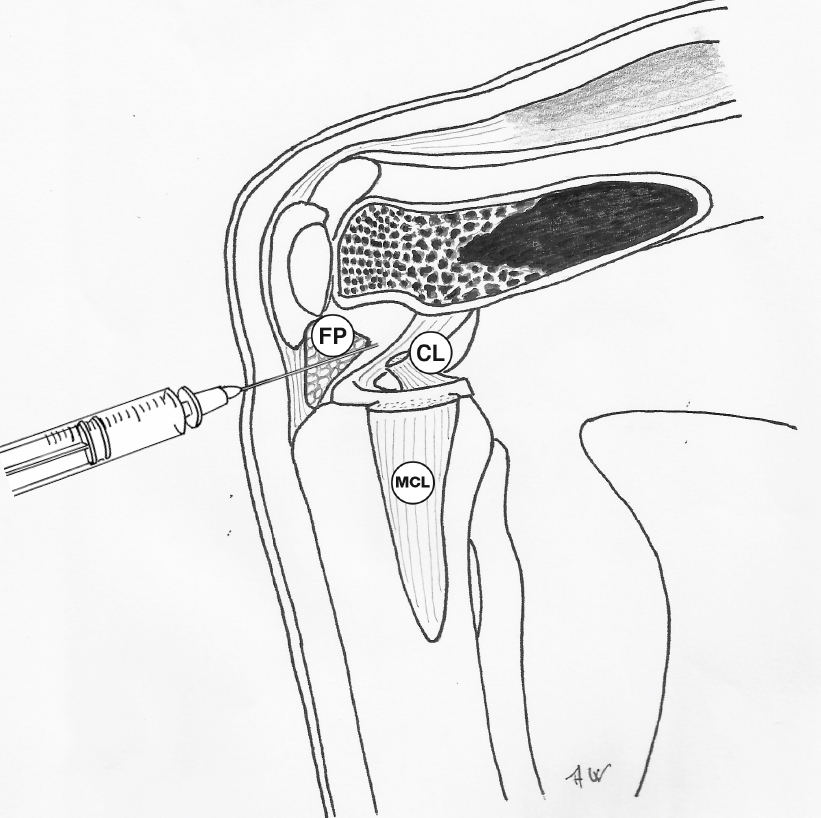
Anterior injection of the knee joint - anatomical diagram (lateral view):
Notes:
- Baker's cysts are swellings present in the popliteal fossa and are associated with knee joint pathology
- treatment of the cyst should be directed at the precipitating joint pathology itself and so any injections for Baker's cysts are via the following approaches
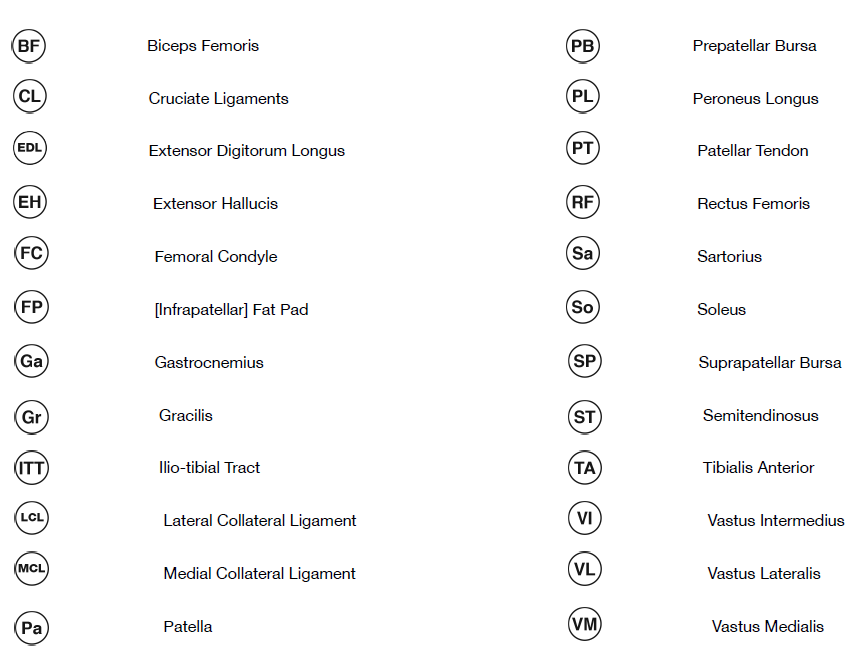
Key to acronyms:
Reference:
Related pages
- Lateral approach - aspiration or injection of the knee joint
- Medial approach - aspiration or injection of the knee joint
- Anterior approach - aspiration or injection of the knee joint
- Pes anserine bursitis
- Injection or aspiration of pes anserine bursa
- Prepatellar bursitis
- Injection or aspiration in prepatellar bursitis
Create an account to add page annotations
Add information to this page that would be handy to have on hand during a consultation, such as a web address or phone number. This information will always be displayed when you visit this page